This is an opinion piece. Its main claim is that the ACA requires denial rates to be available to consumers but they aren't.
Additionally, it reports that denial rates have increased 10x in 10 years, based on the following chain:
- "UnitedHealthcare nixed 1.1%, Humana 1.9%, Aetna 1.5% in 2013, per the American Medical Association."
- "By 2022, major insurers were refusing to pay, on average, 15% of claims, according to a national survey of hospitals and health-care providers by Premier, an insurance consultant."
- "The figure continues to shoot upward, with some companies today denying almost _half_ of all claims, according to researchers at the Kaiser Family Foundation."
Furthermore, "few people appeal, but of those that do 41% obtain a reversal", which suggests the denials may be unfair.
I certainly would like to know the denial rates when selecting an insurance provider. As the article says, "You aren't really insured if your insurer can deny valid claims with impunity."
Given that the ACA requires this information be provided, it certainly ought to be provided. Then we'd have a much clearer picture.
It's an opinion piece on a news site known for inflammatory articles but it reports some interesting information. It would be much nicer if it included references to the research it's based on, but it seems pretty reasonable to me.
Excellent summary. I'd like to address the denials in particular.
As the article says: "No industry malfeasance could ever excuse murder."
With that in mind, we should remember that every death that happens because a valid lifesaving claim was denied is a kind of murder, and no amount of fraud could ever excuse denying valid lifesaving claims.
The stakes are too high: all claims should be approved, then adjudicated later. Fraud should of course be punished severely (with prison, not merely returning the money), but no one should die to protect insurance companies from fraud.
I think you're mixing up terminology here. When a claim is submitted the care (lifesaving or otherwise) was already delivered. You might be thinking of prior authorization, where a provider asks an insurer for advance approval before delivering care. If a payer denies a prior authorization request then some providers will refuse to deliver care unless the patient has another form of payment.
Fraud is only a small part of the systemic problems. There is an enormous amount of waste and abuse by providers who deliver treatments that are ineffective or unnecessary or excessively expensive. The dominant fee-for-service financial model incentivizes over treatment. We can argue about where to draw the line but payers (whether commercial or government) have to push back on this to keep the system from collapsing. Healthcare is already ~20% of the US economy. It can't continue expanding, we simply don't have the resources to pay any more. Every other country rations care in some way; no country delivers unlimited lifesaving care to everyone.
The German state is also helping public health insurers hide their dirty secret: in hundreds of thousands of cases, denials were legally flawed and the cases have to be reviewed. They refuse to do so on the behest of politics as a small number of cases will turn out to be intentionally negligent homicides caused by public officials.
A site properly presenting the facts is due for launch in the lead up to Germany's upcoming federal election. Until then, you can find a teaser here:
Any claim related to outpatient treatment which outside the ordinary requires prior approval there. You cannot opt to pay in advance and seek reimbursement later.
In the state of Bavaria the doctors at a government agency have been practicing without a medical license going back many years because their supervisor let this slide. I discovered her problem randomly in the course of litigation and it impacts probably a million case.
The person responsible for her staff of hundreds lacking a current medical license was later hired to lead the qualifications department at the medical board. That is, after I got her fired from her position and then from a job at a hospital (a felonious psychologist is unacceptable risk for patients). Politics would prefer to see her problem covered up.
There's an easy solution to this that the Federal Employee Program (aka FEP) [0] uses -- regular, external accuracy audits.
The relevant metric to customers isn't "What percentage of claims are denied?" given the substantial amounts of medical claim fraud.
It's "What percentage of claims are denied... that should have been approved?"
So you regularly audit a random sampling of denials, publish the results of that audit transparently, and provide a financial incentive for insurers to keep their numbers below a certain threshold.
It's worked pretty well for FEP -- to the extent that FEP insurers typically have segregated operations from the rest of the company and do much better on denial accuracy and other metrics.
Wrongful care denial should be considered a serious felony on par with assault with intent to do grave bodily harm. It should be a veil piercing crime that exposes every insurance company employee involved in denial to personal legal jeopardy should they wrongly deny claims. Reasons for denials must should be required to be extremely detailed and provided to the institutions requesting coverage. Upon receiving a denial, the health care institution should be able to evaluate the denial for validity and choose to refer the denial to local prosecuting attorneys if the denial is medically unsound.
It would harm profits and maybe give the idea that an LLC doesn't give you license to break the law with impunity. The veil piercing aspect especially would be a major departure from how corporate liability currently works.
I think the biggest barrier is that it inconveniences the powerful to benefit the masses.
Hasn't in the FEP program. Mostly because there's no incentive: doing so helps your competitors as much as you. And it's more profitable to invest those dollars in hitting KPIs.
These "bolt on" type of solutions work but they also raise the costs. Already the administration costs of insurance are through the roof. The system is as inefficient as humanly possible. Hospitals needs hundreds of administrators and billing specialists just to make insurance work - never mind the patient and doctor time lost.
And now, we also pay to audit insurance? It's too much money burning.
This shouldn't be done by the private sector, period. The reason our costs are so insanely high is because of insurance the sheer inefficiency it brings to care.
It seems you've answered your own question - they'd be significantly lower with single-payer.
But to expand, the US has, by far, the highest cost per capita for healthcare at just a bit over 12,000 dollars a year when compared to similar countries. A large part of this is due to our inefficient system, in which administrative costs are astronomically high:
"administrative expenses account for approximately 15% to 25% of total national health care expenditures, an amount that represents an estimated $600 billion to $1 trillion per year of the total national health expenditures of $3.8 trillion in 2019."
There's multiple fundamental problems with the healthcare system that causes this. Again, these problems are fundamental, meaning they cannot be resolved within the constrains of a private sector insurance industry:
1. Insurance billing complexity is extremely high. There are thousands of insurers nationally, and providers are forced to navigate through that to provide adequate care. As a result, many private practices have gone out of business, because doctors spend more time managing insurance than patient care.
2. Insurance has an incentive to deny as many claims as possible. There's simply no way around this fact - the only way to remove this incentive is to remove insurance.
3. Insurance is not transparent to consumers and consumers typically have little to no choice, killing competition and allowing price gauging.
4. Providers are incentivized to charge as much as the most premium insurer in their area allows. For example, if insurer X covers 650 dollars for a treatment but insurer Y only covers 150, then the provider must charge 650. Otherwise, they leave money on the table for patients with provider X. This means that competition in the insurance space doesn't lower prices - it can only raise them. Yes, as boutique plans for employees such as CEOs gets better, your care gets more expensive.
It's a question of what we want to measure. There's a metric that represents how much a claimant sees in unexpected costs due to denied claims vs impact on care from the insurer.
A denied prior auth results in no unexpected costs but perhaps a change or delay in care.
A denied claim to an in network hospital may result in the provider losing revenue but nothing for the claimant.
I think we need more thorough analysis. Are the denied claims denied in error? The appeals success rate probably indicates that most of the appealed denied claims were denied in error... but appealed claims are a biased sample of denied claims, so it doesn't tell us much about the overall denied claims.
In my experience, I've seen some denied claims, because the provider submitted a wrong code. Then the provider submits a new claim with the correct code and it goes through.
Given the proliferation of plans, and their sometimes conflicting requirements on medicial coding, I could see that being a big driver of denials increasing over time. As well as a driver of increased administrative costs for providers and insurance companies.
"A key congressional committee asked insurance giant Cigna on Tuesday to provide corporate documents so that lawmakers can examine the company’s practice of denying health care claims without ever opening a patient file."
From the patient’s point of view, it all looks the same. Treatment that should be covered gets denied.
It sounds like the insurance companies have a strong incentive to make their coding and requirements as complicated as possible to increase the error rate so they can deny coverage. I don’t think they should get a pass for those denials.
I don't doubt that numerous doubly legitimate claims are denied.
What I want is a sense of what the breakdown of the denied claims.
Ex: company sends a list of all denied claims. Auditor picks 100 randomly, gets the files for each and researches those denials to classify the denial as reasonable or not and whatever other categories apply.
In December 2021, the American Hospital Association issued the following statement regarding United Healthcare's plans to closely scrutinize medical claims for ER visits. [0]
UHC subsequently reversed itself and delayed the plan for 6 months. That was in 2021-2022. It's now 2024-2025.
Around that time many insurers, not just UHC, began implementing AI-assisted claims adjudication. It was a bumpy ride with a steep learning curve and probably took a couple of years to fine-tune the algorithms and learning models.
Especially as the Covid-19 claims tsunami subsides.
No matter tho', every claim paid is considered a loss by insurers. Every claim denied is considered a small step towards mitigating those losses.
In the U.S., medical reimbursement is a push and shove, shove and push battle fought inch by inch with high-speed data systems. It has been that way for a long time.
That's simply not how the system works. For the most part, medical insurers no longer provide much real "insurance" in the sense of bearing risk. Instead they mostly act as administrators for employer self-funded health plans. Since insurers are subject to an 85% minimum medical loss ratio, every paid claim is actually a gain because they get to take up to 15% from a larger revenue stream. The majority of the pressure to tighten coverage rules actually comes from those large employers since they're the ones ultimately paying the bills.
It shouldn't even be legal for health insurance providers to deny claims. It's essentially them practicing medicine without a license, because they're making calls about what healthcare a person needs or doesn't need, only a person's doctor(s) should be able to make those decisions.
Agreed. France, Germany, and Japan have health systems similar to the ACA, with the following differences: insurance is nonprofit with an effective mandate, there's a national price list for medical services, and claim denials are prohibited for anything on the list. Germany has an especially effective digital system that guarantees payment within a week.
All three systems get better health results than the US, by measures like survival time after diagnosis of major disease. And all three spend a significantly lower percentage of their GDP on healthcare.
The other side of that is that some expensive services and drugs are simply unavailable in other countries, or are very tightly rationed. The USA has higher 5-year survival rates for most types of cancer than France, Germany, and Japan. I'm not saying that the US system is better overall, but it does do some things extremely well. We should make sure that any reforms don't sacrifice our unique advantages.
I'm not sure how implementing a system like Germany or Japan wouldn't impact those things at all. Why aren't Germany or Japan equal to the USA in 5-year cancer survival rates? Their systems optimize for different priorities, and those involve trade-offs.
So no, it obviously doesn't go without saying. If we want to cut overall health system costs or improve access then we might have to accept some reduction in service quality, at least for the most expensive stuff.
Perhaps because the US is the home of a number of prestigious colleges and to be with your peers you have to relocate there? You act like the broken healthcare system is the only possible explanation for cases where the US provides better care, but I'm yet to see that proven. Intuitively it doesn't track because many of the issues with the system don't pertain to things like intensive cancer care but to simple things that are of the exact same quality in countries with better systems, such as insulin where the only difference in the US is the price.
Not to mention, your comparison on cancer survival rates is flawed. The US system drives many people with cancer to be completely unable to afford treatment, which I doubt you've factored into your survival rate number.
Well now you're just making things up. It's not my cancer survival rate number, it's the number published by the CONCORD programme in the London School of Hygiene & Tropical Medicine. If you had bothered to read the article I linked above then you wouldn't need to doubt because you would know exactly what they factored in.
I did check it, it does not appear to mention this factor at all. I would assume then that they are focusing only on individuals who were able to actually get treatment, since this seems to be the survival rate among patients in treatment.
It seems to me that should then be handled by the legal system or perhaps the licensing boards. That is to say, the insurance companies should be forbidden from denying coverage and if they believe that something is going on then they can alert the police or take the doctor to court.
That's simply unrealistic. Medicine is more of an art than a science and most treatment plans fall into gray areas. While insurers do file formal complaints with authorities when there is clear evidence of fraud (like a single provider billing for more than 24 hours of patient encounters in a single day), there is an enormous amount of waste and abuse by providers which can't be proven in court as fraud. The fee-for-service financial model incentivizes over treatment.
The fundamental problem here is that demand for healthcare is virtually infinite while supply is limited. Healthcare already consumes about 20% of the US economy and there is no excess capacity to expand it further without dragging everything else down. We can make some things more efficient and reduce administrative burdens but ultimately we have to draw the line somewhere and ration care. That's going to be true regardless of whether we have commercial insurers or socialized healthcare.
Most doctors are not very rich at all, upper middle class. I make more than many doctors I know as a software engineer, and this doesn't even take into account their debt.
Care is expensive because of insurance. Hospitals needs hundreds of administrators and billing specialists. Very little of that money goes to the doctor.
Doctors deserve to be rich. They do incredibly specialized work where the outcomes are extremely critical, to put it mildly. I don't want doctors performing unnecessary treatments to line their pockets, but I don't think we're actually in danger of that.
The difference between a rich doctor and a rich insurance exec is that the doctor helps people, and the insurance exec makes their money withholding necessary care from people, in effect torturing and killing them.
This is the problem with insurance in general. The incentive of insurance is at direct odds with patients and doctors.
It's a tug of war, and even if insurance "loses", it doesn't matter, because you lost trillions of dollars in that tug of war. It's artificial inefficiency caused by privatization, very much a Dark Night burning a mountain of money situation.
Yes, insurance companies deny claims, but this is mostly because they don't have the money to pay for things most of their money is spent on care in the first place: they're forced to optimize and people get hurt in the process. Providers do far more damage.
UHCs profit margins are only 6%, their operating costs are extremely low[0], and if you look across G7 insurers in the US pay more than the government does in every country but France![1] Compare this to HCA which makes an average margin of 10% with far higher administrative costs. The CEO of HCA makes $20M, Brian Thompson made $10M by contrast.
This is not to say we (and insurance companies) don't spend astronomically more than other countries: providers are to blame for this, and I have seen their nonsense first hand:
- They keep people alive overnight to charge insurance more
- Some hospitals use ML (!) to optimize ICD codes for billing. Most do this by hand: there's literally a job and training to be an ICD coder.
- They allow people to deteriorate (e.g. dialysis) to charge more (no preventative care.) I have seen a hospital only provide preemptive care to patients at risk of dialysis because they were part of their own insurance pool
- Their administraive expenses are far higher.
- They test and provide unnecessary care.
- Physician shortage is in part caused by limited residency spots, a dumb bachelors requirement, and high tuition costs. These barriers to entry are imposed by physicians.
- Uneccesary tech and equipment upgrades (e.g. we need to replace your knee with a new knee)
- Having to deal with tons of different insurance companies: not their fault but they don't know how to handle this efficiently.
Because customer-insurer relationships are the only side of the healthcare system that most people see, they're oblivious to what are actually pass-through insurer-provider issues.
As you said, the reality is that insurers operate with pretty reasonable margins and incredibly meager per-claim overhead costs. They're stuck trying to make 2 + 1 = 2.
If the finger should be pointed at root causes in the US health system, it should be at:
- Providers overbilling (particular in certain specialties)
- Medical schools, for charging too much and under-expanding capacity
- The federal government/Congress, for failing to expand residency funding to increase supply (especially in generalist provider categories)
What’s the source of limited supply of doctors meme? Is there a good rundown somewhere?
Because anecdotally, among my friends, I’ve never known someone to not make it through the system to practicing medicine who wanted to, but I do know several who persevered despite being real idiots. I don’t see how opening the pool wider would lead to better care.
1. There is a cap on the number of doctors that the US can churn out since Medicare funds most of their training. That number is 140,000. This inherently limits supply. This is the biggest issue.[0]
2. There are limited spots in certain residency programs due to how competitive they are. Ergo those specialties are artificially more lucrative. Dermatology is a good example.
3. Becoming a doctor is temporally arduous: 11 to 15 years! Why the hell do people need to spend four years of time and money on a bachelor's degree instead of entering a medical program directly?
4. Becoming a doctor is financially arduous. You will be in debt for four years of undergrad, then four years of medical school, and then you'll be paid garbage for 3-7 years of residency. High interest rates exacerbate this.
5. Residency is hell.
6. Working in a hospital is often hell. Burn out is very real.
7. There are many, many professions which provide a far better standard of living.
Agreed. There are a few schools now offering accelerated Baccalaureate-MD programs in as little as 6 years so expanding those to more schools would be a relatively simple way to cut education costs.
We can also expand access to affordable primary care by shifting routine services to physician assistants and nurse practitioners. Physicians should be reserved for more complex or higher risk cases.
1. This is true sometimes, but still privatization and insurance's fault. Hospitals have a motive to charge insurance more money. Public healthcare doesn't have this problem.
2. Administration and billing is ludicrously expensive because of insurance. Thousands of insurers with their own processes breeds the most inefficient and broken system you could possibly imagine. The solution is removing the market, i.e. having a single payer. Boom, administration costs disappear.
3. Preventative care is rarely paid for by insurance. In addition, many patients simply don't do it. It's easy for a smoker to get treatment for COPD, it hard for a smoker to stop smoking. That's just how it is.
No matter how you slice the healthcare problem in America, it undebatable that private insurance must go. The inefficiency it creates is absurd and it's why our healthcare costs are through the roof.
Not only do we pay much, much, MUCH more per citizen for care, but our care is also lower quality as compared to the rest of the west.
Expanding, essentially the US has the worst of all possible worlds.
Most provider costs are obscured / complicated by insurers sitting in the middle of transactions.
If they weren't, providers wouldn't do some of the all-but fraudulent coding shenanigans that have become normalized. But overbilling a faceless insurer is fine.
And likewise, patients would have an incentive to shop around for the most cost effective services, instead of no one in the system being able to proactively say how much something would cost until the insurance claim is submitted and processed.
USA Anti-trust is on life support and there is generally very little political willpower to disentrench incumbent capital interests.
Wealthy lobbyists for providers and health insurance companies prevent any change basically.
Also misguided American exceptionalism whereas people think the healthcare standards will go down significantly if there is a public option (as if they weren't already down for the things people can actually afford).
Sounds like the business model they’ve decided to use might not be viable.
I mean, actually it makes sense. Their job is to pay for expensive procedures, sometimes quite urgently needed. They can’t really ethically insert themselves into the decision making process, so if these companies were run ethically they’d be signing themselves up for unlimited risk.
Please allow me to counter, from the perspective of someone who owned a medical practice for much of my adult life:
- The ACA limits the amount of money, as a percent of revenue, that insurance companies collect as profit. If they wish to increase profit, their primary option is to collect higher premiums and pay more benefits.
- (No experience with keeping someone alive overnight. I'm sure it's happened and couldn't disprove it in any case.)
- Of course they have optimized billing. The current fiasco has byzantine rules for payment. For instance, you know how your dermatologist offers you smoking cessation and weight loss classes? That's because if they offer it to you, insurance rules allow them to bill the encounter as an enhanced care visit which pays more. This isn't an exaggeration. The insurance rules say "we'll pay you an extra 30% if you ask about their smoking and weight". The doctor can earn more simply by following those rules. Again, of course providers do this! If my boss gave me a 20% raise for asking him each morning if he'd like me to make him a sandwich, even knowing he hates breakfast sandwiches, you bet I'm doing it.
- That's complicated. If a hospital violates the insurer's rules, they don't get paid for seeing the patient. Yes, the situation you described is horrid, but no provider can afford to write off every patient. It's the insurers who said they wouldn't pay until the patient is seriously sick.
- Surveys have shown that as much as 60% of small practices' management overhead involves staffing people to deal with insurance companies, process claims, optimize billing (see above), negotiate pre-approvals, and so on. They have higher overheads because the insurers require it, not because they want to.
- Well, according to the insurers trying to weasel out of paying for it. For example, a patient came to my wife with an obvious soft tissue injury. She ordered an MRI to diagnose it. The insurer refused the approval until my wife took an X-ray first because it's cheaper. X-rays also don't show soft tissue injuries. (Don't correct me; I know the exceptions here and they're not relevant to this.) So it was the insurer who demanded my wife perform a wholly useless test before they'd pay for the effective one.
- I'm not willing to lower the quality of physicians. Other studies have shown that the lack of upcoming doctors is due to fewer people willing to put up with the insane stress levels for mediocre pay. The stereotype of a doctor heading out at noon for an afternoon of golf are largely over for nearly all specialties. Frankly, there are many jobs that pay better with less stress and less personal responsibility.
- That's laughably wrong. No one gets a new knee for the fun of it. It's a major surgery with long and challenging recovery that people get because they're otherwise unable to function normally.
- There is no way to handle this efficiently. It's an utter morass.
- I'm not willing to lower the quality of physicians. Other studies have shown that the lack of upcoming doctors is due to fewer people willing to put up with the insane stress levels for mediocre pay. The stereotype of a doctor heading out at noon for an afternoon of golf are largely over for nearly all specialties. Frankly, there are many jobs that pay better with less stress and less personal responsibility.
This assumes that the things being done now are meaningfully contributing to the quality of physicians vs various proposals.
It's also probably a mistake to measure the quality of the doctor vs the quality of the care that is delivered. More doctors that are less stressed and can spend more time on each patient could easily outperform a smaller group of "better" doctors.
> Otoh some medical providers like to over bill and over treat.
This is true to some extent, but the share of medical providers that over-bill and over-treat really doesn't justify the way the insurance industry does business. It's a false equivalence.
Yes, but in my opinion it falls to the patient to figure out the details and absorb the risk. That's the messed up part. That insurance providers and medical services might disagree on pricing or whatnot is an inevitability. What's not fair is throwing ordinary people under the bus to deal with it, which for many reasons is risky and can ruin lives.
Stop speciously muddying the waters by either intentionally or accidentally making spurious arguments for these unethical sociopaths.
I’ve seen this argument made on this website a lot, and it always conveniently omits the vertical integration of these insurers wherein they are the providers too.
The DOJ is literally, actively, suing to block a merger between united healthcare and a provider.
It's not clear that vertical integration is necessarily bad for consumers. For example, Kaiser-Permanente is a huge, vertically-integrated "payvider" which both sells insurance plans and also delivers most of the treatment for plan members. They generally do a pretty good job at a competitive price.
Both the payer and provider sides of the healthcare industry have been consolidating for years. Insurers merged to gain more negotiating power with providers and drive down costs. Providers responded by merging (or selling to private equity funds) to gain more negotiating power with insurers and maintain high rates. Government mandates on back office technology also incentivized provider consolidation due to economies of scale. In some areas now a few major provider organizations effectively control the market and payers are essentially forced to pay high rates in order to maintain sufficient networks. So, the logical next step is for payers to mimic KP by building their own captive health systems. Every major payer is pursuing this strategy to varying levels; it's not just UHC.
I'm glad to see this phrased this way, because that was something I felt but hadn't articulated consciously. It's literally private accountants making healthcare decisions.
All large health insurers employ many physicians. You're not wrong that they may not have all of the evidence but there is a lot of licensed medical knowledge available to all Payors.
That’s the crux of it. I didn’t visit with any of my insurer’s staff, like I did with my own doctor. How are they making treatment decisions without ever having seen the patient?
Worth noting: neither major Presidential candidate, nor the news media, made health care a focus of the recent election. The issue was almost ignored. And neither major political party offers much: the Democratic establishment will defend the Affordable Care Act to the death (literally in this case), despite the fact that it's not particularly affordable, becoming more unaffordable over time, and it continues to enshrine and subsizide the ruthless for-profit insurance companies. On the other hand, the Republicans paint any kind of government involvement in health care as "Communist", despite the fact that the entire rest of the civilized world have more efficient, effective, and compassionate health care systems heavily regulated by the government.
I think it's a sign of deep American corruption that we can't even have this public debate without a salacious murder occurring.
The affordable care act is the most reasonable path from the current american system to a system on par with other first world countries. This especially given the sort of republican opposition it's liable to face. It's current form is due in substantial part to the republicans gutting it, so you can't really blame the dems for it not working very well.
John McCain, a Republican, famously voted to save the ACA during a time when the Republicans had a Congressional majority, even though his health was failing. He died shortly after the vote.
I was talking about the 2010 passage of the ACA, not the 2017 repeal attempt. The 2010 legislation was written by Democrats. Moreover, since as you mention, the Republican repeal attempt failed, it can't truly be said that Republicans have "gutted" the ACA. It is true that for some (dumb) reason the ACA gave significant power to the states, which has been abused by Republican governors and legislatures, but that was entirely the choice of the Democrats who wrote the ACA.
She says that you can’t find denial rates for specific providers then she gives denial rates for specific providers. I’m not sure if she cited a source. I’m curious where her data comes from.
Let the health insurance companies deny claims. But then let the medical providers duke it out behind the scenes! Leave patients alone and don't send them bills six months later.
The problem today is the insurers, hospitals and doctors put the patients at the center of the fight.
Insurance denied? You pay patient.
Insurance didn’t pay doctor enough? You pay patient.
Hospital not in network? You pay patient.
I think patients would see it as an improvement if hospital said upfront to go somewhere else as insurance won’t pay. If they knew insurance would pay at the right hospital than it would be better than today’s situation.
Assuming you are a coder lets see how that works for you..
Someone comes to you saying they need a website. You say "absolutely ... clearly you need one!". So you build it.
The decision to pay you however comes from some 3rd party who says "denied". Now the customer keeps their site and you don't get paid.
Will you stay in this coding business?
The real solution is a public health system. Which has issues (apply queuing theory, because you will have to wait for the limited resources you are niw denied) overall it is better though since it can in theory be optimized as a whole.
Of course not legally, but I think there's a philosophical exercise here for ethicists to debate the boundaries and efficacy of community self defense.
One thing that will help greatly is to regulate hospitals into having an umbrella of "services" that allows "private" operators BUT those operators have to be covered by any insurance that wants to work with the hospital rather than these 3 nurses in one pay center, this surgeon in another, assistant surgeons in a third, and the anesthesiologist so far out of network he laughs and isn't part of any HMO, PPO or anything else.
>"An appeal means coaxing your doctor and staff to spend hours filling out forms and making repeated phone calls to joust with an insurance company employee."
The hospital where I receive my cancer treatments once told me "don't worry, our Denial Team is handling this."
They have a Denial Team. That is to say, insurance companies are imposing cost overheads on providers and patients due to their illegitimate profit boosting tactics. And our government can't be bothered to enforce the ACA's basic requirement to track and report denial rates.
>"No industry malfeasance could ever excuse murder.
"Period."
And yet, that's what it took for our media to start reporting on this? We have some real problems in this country, and a corporate news media asleep at the switch, or at worst complicit, is one of the most serious.
If you're seeking coverage for lung cancer, but you chose to smoke, denied.
If you're seeking coverage for type II diabetes, but you weigh 400lbs, denied.
If you're seeking coverage for cancer because you got unlucky with a cosmic ray incident on your DNA, approved.
If you're seeking coverage for a liver transplant because you refused to put down the bottle, denied.
If you're seeking coverage for injuries from an auto accident that was not your fault, approved.
I will NEVER understand why this type of blanket policy is so controversial. Cover bad luck, do NOT cover personal choices. It will fix not only costs, but the moral hazard endemic to the current system.
Or, AT THE VERY LEAST, allow prejudicial adjustments to premiums for fatties, smokers, and alcoholics.
- Health "Insurance" middleman mafia should not be the default b/w me and my doctor
- Health Insurance should only exisit for Catastrophic events (big surgery, cancer etc)
- Get rid of the regular Premiums, CoPays, Deductible, CoInsurnace, In network/Out network Bullshit.
- For catastrophic events, we pay a premium (much smaller than now)
- All hospitals and Doctors must offer an advertised/displayed Cash Price. No exceptions. Fine heavily if they hide
- Let me pay cash for a regular doc visit.
- Govt can subsidize for poor people (exdtension to medicare etc ??)
That's it. Problem Solved. This will remove so much BS, middleman stuff, overhead and with a competitive market, prices will drop significantly. Doctors will be happy not dealing with Insurance for everything.
I would argue that people already dread going to the doctor because you still have to deal with all the insurance garbage. Remember that even with a copay, you still could get a bill after the visit depending on deductible.
In 2022 I was denied full insurance payment of a routine, preventative echocardiogram at Stanford Healthcare to monitor my heart issues. I was balance billed $5000+. The insurance company was HealthNet. The policy clearly indicated full coverage of preventative procedures, without a deductible. They said they did not recognize the procedure as preventative. Fuck them, I know better about what's preventative and what's not than them.
I argued the shit out of it, dozens of e-mails, hours of phone calls, and it was eventually sent to debt collectors. I wrote back to the debt collectors that it wasn't my debt and to stop contacting me. I reported it to a couple of government agencies as well to give them more headaches. I did not pay.
In 2024 it was written off as uncollectible.
(a) Use a virtual mailbox with your health provider so that they don't send debt collectors to your residence. Do not give them your residential address.
(b) Use a virtual phone number with your health provider so that the debt collectors can't call you. Their only option will be mail and that leaves a paper trail which you DO want. NEVER communicate with a debt collector by phone.
(c) Freeze your credit reports with all 3 bureaus so that they cannot use your mailing address to find your residential address.
(d) If they do somehow find your residential address, do NOT answer. Only communicate by mail.
Disclaimer: IANAL, account of personal experience only
Under the Affordable Care Act (Obamacare), there is a very limited and specific definition of preventive care services which health plans are required to cover. An echocardiogram is not on the list.
In your particular case it might have been medically necessary, but not legally classified as preventive. This is a huge hassle for patients because the nuances aren't obvious or clearly documented. It's likely that Stanford Healthcare erred by failing to obtain the necessary prior authorization from HealthNet before performing the procedure.
Since 2022 there are some legal protections against balance billing. Although those might not have helped in your case.
The insurance companies don't have medical training either. I know far, far more about my body's medical situation than them.
Doctors and medical research may supply me with additional medical knowledge, but the insurance company can go to hell. They don't know a damn thing about any of this.
(a) I believe medical debts don't affect credit scores for a long time.
(b) I believe medical debts are required to have complete erasure from a credit report if cleared so if I actually needed my credit score to buy a house or whatever I could take the $5K hit to restore the credit score at that time.
(c) I sent them a formal letter disputing the debt, which I assumed means they can't just take it to the credit agency, they'd have to go to court with me first. (Again IANAL, I don't know how accurate this is.) In any case I was mentally prepared to spend $10K on lawyers and court and give them a absolute hell of a time than pay $5K to pay for healthcare I shouldn't need to pay for. I made it VERY CLEAR to the debt collectors that I was ready to pay for lawyers.
(d) For the forseeable future I don't think I need my credit score for anything. I don't plan to borrow money.
Fwiw, in New York state, medical debt is prohibited from being reported on the credit report or from affecting the credit score. California has also passed such a law that takes effect soon.
New York's law focuses on prohibiting healthcare providers and related entities from reporting medical debt, while California's law directly restricts credit reporting agencies from including medical debt in credit reports.
As opposed to a Medium blog? If source material and reputation is the concern.
Many online papers have pay walls. There are similar articles criticizing health care denials from other sources, feel free to post them. They're not all discussion material nor even readable.
And if the writer did a poor job, poke a hole in the argument.
I was just denied a colonoscopy as not medically necessary by UHC, coincidentally three days before their CEO was killed, because they don't want me to have anesthesia to do it; they argue I should be awake.
When I called to refute the denial, which was denied, I asked them to find the person, if it was a person, who denied it and shove a tube up their ass without anesthesia and then reassess whether it's medically necessary to have a colonoscopy without it.
I'm 45. Colonoscopies are a thing. I had a friend die at 52 two years ago after he was diagnosed with stage IV during his first colonoscopy. I spent many of his last days watching him struggle to survive; I don't want that to happen to me just because UHC charges me $2000/month in premiums and denies basic service because they need to pay their executives too much money.
I'm an anesthesiologist. What they denied was paying me to do it. You can still get "moderate sedation" from a nurse - a benzodiazepine and opioid.
Patients strongly prefer having what amounts to a general anesthetic; your chances of recalling anything are low either way, but propofol results in a much faster recovery to full consciousness afterward.
Go gain 100 pounds and develop sleep apnea. Then they'll approve it.
Propofol (or equivalent) is a must. I know people who have had a colonoscopy without it, and have regretted it due to significant pain.
Note that they approved the colonoscopy, just not the anesthetic. Also, to get approval for a colonoscopy, one just needs to have persistent intestinal pain or note that they have a history of polyps.
I am well aware of the colonoscopy rules. I struggle with them when patients who would not meet the standard are scheduled with us because they are employees of the hospital and it will not pay for care outside the system. It is one of the many factors that goes into the hospital’s subsidy to my group. Most of these are too ill to be done in a non-hospital facility - though most do fine and go home, there are some we have to admit overnight for observation.
It is almost universal that hospitals pay from their fees for part of the anesthesia services because the direct reimbursement we get is so low.
You can get one at 45, no questions asked, or you can claim you had a bloody stool.
As far as pain, that’s hard to measure. Procedures that are done under sedation or anesthesia in the US are done in other countries with little or nothing. I had all of my wisdom teeth extracted and all of my dental fillings done under local anesthesia only. It was fine. I don’t need gas, I don’t need sedatives.
> I was just denied a colonoscopy as not medically necessary by UHC, coincidentally three days before their CEO was killed, because they don't want me to have anesthesia to do it; they argue I should be awake.
It sounds like something is getting lost in translation. Presence or absence of anesthesia does not change the medical necessity of the procedure.
> I'm 45. Colonoscopies are a thing. I had a friend die at 52 two years ago after he was diagnosed with stage IV during his first colonoscopy.
Without wading into the specifics of your situation, there's not great evidence justifying colonoscopy for normal people without family history at age 45. The USPSTF just kinda lowered the threshold based on crappy (pun not intended) observational data. And if you look at their recommendations, they actually don't recommend colonoscopy, specifically -- they just recommend "screening" [1] which includes FIT, DNA testing (again: not great evidence here), or flex sig, which is done without anesthesia, and all of which are cheaper than colonoscopy. It's a huge debate.
Anyway, I absolutely don't want to reflexively defend the health insurance industry in the US, but one the reasons we have skyrocketing health care costs in this country is because people are doing expensive procedures when cheaper ones would suffice.
When my doctor recommended mine, she said that they could do screening but if they found anything, they would have to do a colonoscopy and then it wouldn’t just be covered as screening (since it was an incident rather than preventive at that point). She said it was better just to get the colonoscopy due to health insurer rules.
If they find something suspicious during the colonoscopy, they won't bill it as a free screening anymore and you'll be on the hook for it. Ask me how I know.
No regrets about getting screened though. It saved my life.
Sorry, I meant: if you do a non-colonscopy screening first and they find something, the follow up colonscopy isn't covered as preventive. And the non-colonscopy screenings have a higher false positive rate than a colonscopy screening.
Good to know. I was just adding to what you said that even if you don't get a positive result before a colonoscopy, the colonoscopy might not be covered as preventative care. Insurance just really doesn't want to cover it.
> It wouldn’t just be covered as screening (since it was an incident rather than preventive at that point). She said it was better just to get the colonoscopy due to health insurer rules.
Well yeah...it isn't screening then. It's a treatment. So the question becomes whether or not the treatment is necessary. If the prior "screening" didn't show definitive evidence that the treatment is necessary, then...what are you doing, exactly?
I understand that colonoscopies mix up the notion of treatment and screening, but the doctor is basically saying "our screening tests don't work very well, so we should just do the treatment without evidence because they'll pay for that."
Fair enough. I'm making a broader argument than just your situation (which obviously I don't know). The insurance companies are not crazy for trying to control costs on this kind of stuff...however ham-handed their methods.
I get that, but my point is that in health insurance, you're pretty much always going to find someone complaining about being denied for something, even if the denial was completely justified on an evidentiary basis (again: not talking about OP specifically here). Literally every cost-control measure -- even if sensible -- is going to be framed as evil by someone.
A lot of health care is just really expensive superstition. For a more extreme version, consider the phenomenon of "preventative MRIs", which are just lighting piles of money on fire for no reason at all.
I replied to colonoscopy specifically here because the general public has been conditioned to believe that these screenings are medically necessary at increasingly younger ages for everyone, despite the fact that this is not the standard at all in most other countries.
But it's not usual to have an anesthetic for a colonoscopy is it? I've had two without. I was offered a light sedation but then I couldn't have driven home afterwards. It wasn't particularly awful without.
It's it usual to be asleep? I've not really heard of that. Is it a US thing?
I'm not a medical doctor, nor a clinician that does colonoscopies, so I have no idea. All I know is that the clinic suggested by my primary care physician set everything up and UHC denied it 10 days prior to the procedure, leaving me almost no time to work through any sort of processes to effectively change their decision--if it's even possible.
Without any real evidence except a hunch, I think it's because I've already met my deductible for the year and they don't want to pay for the entire thing and they'll do anything they can to avoid having it happen this year and hope I just go away or do it in another year when I haven't hit my deductible.
Same here, just had one in the US and I refused to be sedated as I knew from previous one in EU that it is tolerable. You should have seen the song and dance of the provider trying to convince me to get sedated. In the end they accepted my decision. Afterwards about everybody in the clinic came to see me as if I was a hero of sorts. However,the whole episode gave me a good insight as to why US healthcare is so expensive.
> Anesthesia or anaesthesia is a state of controlled, temporary loss of sensation or awareness that is induced for medical or veterinary purposes. It may include some or all of analgesia, paralysis, amnesia, and unconsciousness.
"General anesthesia" is probably what you're thinking, which is a specific form of anesthesia where someone is put to sleep.
i was actually confused about this for a long time - i always thought my colonoscopies were "general" because i... couldn't remember anything, but all of them were really just propofol "twilight," which is just a deep sleep, i guess? i only learned this when i got a real surgery and had to actually go under general, it's a much more involved thing where you're essentially put in a coma
i'm not sure if it's a US thing but i think especially if they're going to take biopsies you're put under twilight, which is one step below general - i don't remember anything about any of the ones i've had, and wake up later in a recovery room
I'm in US and I've had a single one. It was sedation which induces twilight sleep but I was definitely conscious. I've known many that have had them (ex-partner had stage 3 colon cancer and had/has them on the regular) and it was always sedation.
I dunno if it's unusual? I had mine done recently, 49 years old... seemed like a given that I was going to go under? (I'm pretty sure I prefer it that way?)
Also UHC fwiw, but went through my local provider group, etc...
It is extremely common in the US. The only people who get colonoscopies without any sedation are those who want to be able to drive themselves home afterward.
We have people - covered in tattoos - who insist that they are terrified of needles. And that they want drugs before any even mildly painful procedure, like placing an IV.
I've done a colonoscopy without anesthesia before... it was a non-event. This is pretty common from what I understand elsewhere in the world. Americans are just super uncomfortable with their bodies so I guess we prefer being put under?
> I've done a colonoscopy without anesthesia before... it was a non-event. This is pretty common from what I understand elsewhere in the world. Americans are just super uncomfortable with their bodies so I guess we prefer being put under?
It depends on what they do while they’re in there. If they’re just taking pictures then it’s fine. If they find anything they usually cut it out immediately. I can tell you from experience that having a piece of inflamed colon cut of and cauterized while you’re conscious isn’t a “non-event” as cool as it might be to watch on the monitor.
Good god. I went to get one, and in the pre-screening, the anesthesiologist asked if I wanted to be awake for it. “Doc, I don’t want to be awake, I don’t want to feel a thing, and I don’t want to remember a thing. Put me out.”
Requiring people to be awake is a good way to guarantee they don’t get the procedure. Which mathematically makes it far more likely for the insurer to incur enormous colon cancer treatment expenses, erasing their profiteering.
that's insane! everyone should get a colonoscopy, and i believe they're recommending them for people over 40 if you meet certain risk categories
signed up for an account with my real name to share a doc i've been working on for a long, long time now - i've had UC since high school, and have written an extensive guide of what i've learned, if it helps you or anyone else you know who might be getting scoped:
It's estimated by CRUK there are 44,000 bowel cancer cases each year in the UK. Assuming only people over 40 get it, and that's about half the population, the incidence is something like 1 in 800 annually. The rate of "serious complications" for a colonoscopy is about 1 in 300.
Given those numbers, how often should everyone get a colonoscopy?
That's before we get on to the potential harm from a false diagnosis (which is much higher without additional priors).
Yes, absolutely people should pay attention to their bowels and get a colonoscopy when it's indicated. Let's not all rush to get one though unless there's some reason for it.
to be clear, i'm not a doctor or an expert, just a person with gasto problems - maybe to elaborate a little from my original comment: i think everyone over 40 should be screened (with a colonoscopy or other non-procedure testing) for colon cancer, full stop. then, say, every five or ten years depending on the results?
i also believe pre-screening (stool sample testing, mostly) is getting better, which would potentially help categorize who does and does not need an actual colonoscopy in the future
these are all US stats[0], which i'd imagine is a broadly worse-off group than the UK in terms of like, ultraprocessed foods and other risk factors, but this stood out to me:
> Lifetime Risk of Developing Cancer: Approximately 4.0 percent of men and women will be diagnosed with colorectal cancer at some point during their lifetime, based on 2018–2021 data, excluding 2020 due to COVID.
anecdotally, i think with gastro problems there's a lot of individual latitude where serious problems might go undetected, under-reported, or assumed to have a less serious cause - i also think (but do not know) that colon cancer develops slowly, which may mean there's a long potential where it could be caught, detected, or risks flagged early by a colonoscopy, which, to me, outweighs the risks of "serious complications" from the procedure
They should make anyone who denies anesthesia for a colonoscopy drink that awful orange flavored drink you take the night before. This is just like... basic care.
It is really common to be out on full anesthesia for a colonoscopy. I’m confused by your comment. At least in the USA, I think it is standard and they don’t really talk about any other options.
I am in former soviet country. My relative is refusing to go for optional surgery, bcos they would put her under full anesthesia. She already had "too many anesthesias" in her life, and her brain may not take it well.
Anesthesia in many cultures is seen as a "drug use" and avoided. It has several risks, including death. In many cases it includes needle into backbone.
I’ve only been under twice: did a colonoscopy and for wisdom teeth removal. In both cases, it was simply finding a vein on my arm and I was out cold pretty quickly with a weird gap in memory when I came back. It didn’t sound like taking a risk, at least as it was sold to me.
I think we're confusing general anesthesia (not generally used for colonoscopies in the US) with sedation with something like propofol which is pretty common.
They found cancer in my colon during a follow-up for a ruptured appendix, several years before the age for recommended colonoscopies. I recently had one and asked they go light on the anesthesia, so I was in and out. They removed a polyp while I was awake and it was pretty uncomfortable. The idea that you shouldn’t even have that much anesthesia is insane. These people are morally bankrupt and frankly I don’t care what it takes to stop them.
I'm going to be a bit contrarian and say that drinking that awful liquid the evening before the procedure is 100x worse than not doing it with anesthesia. I did my colonoscopy without any anesthesia, and while it's not very pleasant, it's not painful, it's just a very weird sensation.
When all the acceptable solutions are taken off the table, people start turning to unacceptable solutions. It's not good, because the erosion of social institutions will worsen the situation for everyone, but the only way to deal with this is to put the acceptable solutions back on the table. If we don't want to live and die through the inevitable consequences, our government needs to stop the corporate abuse of power that has led to this.
Murder isn't the same as homicide. By definition the death penalty isn't murder, because it's state sanctioned. Self defense, another example of legal killing, also isn't murder and most people who are against murder would consider a death in self defense to be justified and not murder.
Self defense can give mitigating circumstances in some legal systems, but it’s not an ethical joker to kill whoever we self-decreed feels as representing a threat.
For example, we can go into treacherous schemes that pushes our neighbors into paths where the only obvious option they can still perceive as a way to escape our shenanigans is an attempt to kill us, and as they come with this very real intention to kill us, press the button we had prepared to trigger some mortal trap.
> Considering that a lot of innocent people are murdered by the state via jury and trial in the US the distinction isn't very clear imo.
~211 people were killed via trial sentence in the US in the last 10 years [0]. Presumably some of them weren't innocent. In the same time period (conservatively) 8500 were killed by law enforcement outside of the legal process [1].
Both are problematic, but calling <20 people/year (out of a third of a billion people) "a lot" is missing the forest for the tiny sprig of moss.
You could easily argue the opposite is also possible to be true - if by "murder" you mean "killing" in general.
It's quite possible for someone to hold that a killing in self-defense is much more defensible than the deliberate execution even after a conviction and trial of someone who is "no longer harmful to society" because they're locked up.
Maybe. But do you have an example of a society that do both death sentence and provide fair trial plus peers conviction?
Making prevailing the idea that some humans can reach a level of certainty that is high enough to put a death sentence on some people they didn’t even knew before that is telling a lot. Like, we humans never make errors, we don’t have any kind of cultural and idiosyncratic biases, we never have conflict of interest and we can’t be manipulated by miscellaneous social forces.
Murder is bad, and murder en masse committed through institutionalized legitimating mechanisms is thus extremely bad, as as many times as bad as how many people it kills.
Legal murder through institutions never prevented a society to have "random" citizen going awry and kill other people, but it never missed to add supplementary threats to all their citizen.
This. The cognitive dissonance is jarring. And no "that's different!" is no argument. Like it or not, our government leads by example. And the example is not a good one.
This is because the US is not one homogenous system of thought, but rather a mosaic of people with differing views. (This goes for any other country or population for that matter.)
A more constructive observation would be to consider the overlap in groups of people who (1) hold that murder is indefensible in any case, and (2) hold that death sentences are appropriate for crimes. While not sharing that view myself, I could think of a few factors that may lead others to espouse it, such as:
- an implicit trust in authority and deterrents (follow rule, "or else");
- feeling of being mostly immune to errors in the justice system ("this would never happen to me");
- a propensity to desire revenge but only when it pertains to "others" ("I'm a good person, we must punish the bad people")...
Murder is by definition an unlawful homicide. This isn’t just pedantry; it’s the most parsimonious explanation for why someone would support the death penalty and object to something like the assassination.
Until the day we can point to a country that implements a direct democracy with a fair way to obtain citizenship for whoever is involved in its society, all laws will always remain a tool of a minority to arbitrarily rule a majority.
The concern is not whether laws are rights or wrongs, but which privileges and which hurts they reinforce for which classes in the society where the national myth is eager to present them as the applied rules.
> Until the day we can point to a country that implements a direct democracy with a fair way to obtain citizenship for whoever is involved in its society, all laws will always remain a tool of a minority to arbitrarily rule a majority.
For the same reason we might want to distinguish between well functioning government and direct democracy.
First, direct democracy is kind of a pleonasma, that is in its core democracy has to put equals duties and means to all its citizens. It's clear probably why such a system can easily attract masses, as it promises to maintain political power in the hands of those who have to obey it. Note that this definition insist more on duties and means, which is a very different promise from a populist statement on "righteous rights for everyone thanks to a turn key plan you don't even need to investigate on applicability". People certainly are interested with more democracy, so their slavers scam them with all kind of system under the label democracy which never give them these duties and means that you can expect to see attached to an effective democratic citizen.
The initial proposition was that it is pedantry to distinguish between the quality of the killing when the form of governance is not a well functioning democracy - something that would appear to be well established as the US has no issues going into other countries and kill leaders under the argument that it is not democracies.
The question is not so much the quality of the US democracy but to what extend it can even be classified as a well functioning democracy.
The US resembles an oligarchy, and when the laws are written by the rich and profit seeking that will affect how killings are perceived such as killing in the name of corporate profits will become alright.
It's a little different when a jury of your peers convicts you of a crime which was democratically passed by a legislature, versus a lone gunman who feels he is the judge, jury, and executioner.
America is the land of stand your ground laws in which a citizen may legally take a life if they feel endangered. Let's not forget the 1000 or so police kill every year.
In the death row case, the capital punishment isn't murder if you use classic definitions. If you change the definitions then it's only murder if you equate all homicide to murder.
And yes, both the will of the people and tradition can justify capital punishment.
That's fair. And in that vein the current killing of the ceo can not rightfully be deemed a murder as no one have been convicted of such.
But then again, the society apparently defines the quality of a killing - only future history will tell if this is a murder, and thst can go back and forth a lot depending on public sentiment.
Forget gerrymandering, a representative government is impossible as long as the Senate still gives the same weight to the 15 people in North Dakota as it does the 40 million in California.
Not to mention that we happily do extrajudicial assassinations outside of our borders, and the news falls all over themselves to celebrate them.
Everybody knows that plenty excuses a murder, we live in murderous states and in murderous times. The question is whether this murder is excusable, and one's opinion on it is probably dependent on whether one wishes they had that guy's job. Most people wouldn't do it for any price, but plenty would.
> A claim denial that results in denial of life-saving treatment could never be counted as either of those charges.
First-degree murder is when you willingly, and with forethought, plans and carries out the killing of a human. Which seems to me to be 100% what you described.
Denying a claim can not kill someone. Disease and injury killing a person. Claim denial prevents financial support for intervention in resolving a disease or injury. That is not the same thing, and equivocating them is sophistry.
If you’re shot, and I pull up a chair and watch you die without saying a word or helping in any way, especially if I get paid extra for refusing, I’m not sure if I’d call it murder, exactly, but I bet your family and friends would describe me as a killer.
I’d say that not equivocating them is sophistry. In both cases, someone takes a deliberate action that they know will result in an innocent person’s death. I fail to see why the exact mechanism should be so important.
The act of killing a human being is not inherently murder. It specifically communicates an unlawful killing, which the death penalty inherently is not.
I'm trying to figure out if these deaths caused by insurance denials could actually be considered murder. I think they would definitely qualify as being premeditated, but can you consider them "killing"? They are causing death due to omission of expected care, but can the omission of something like medical care be considered the cause of death?
It is weird—I would expect only the folks who make decisions as to which procedures are medically necessary (just doctors ideally) to have a duty of care. But insurance companies are bouncing back procedures are not medically necessary, so maybe we’re due for a re-adjustment in the expectations as to who has that duty.
It is surprising if insurance companies what to sign themselves up for this sort of obligation. But obviously they’ll take all the privileges of the decision making process if we don’t also hold them to the responsibilities.
There are direct measures: someone needs a transplant or something of that nature, refusal is effectively shortening their life and some aggressive prosecutors might craft a case. There are less direct things, I expect a lot of them. say people dealing with long recoveries from things, there are good days and bad days and bouts of depression aren’t uncommon; could antidepressants prevent depression on related suicides? That’s an entire can of worms, people have fallen into depression because they’ve become addicted and can’t kick it, what if it was medical pain killers you’re addicted to? Then suppose some company spent half the funds on ED pills and breast augmentation and some more medically things were denied, you can spin that both ways as they might be doing what the bulk of their customers want. That one is interesting, you could break a bone and have surgical reconstruction and hopefully get a full recovery or maybe you just set it and naturally heal and maybe it’s not 100% fixed, only 85%, there is a substantial cost difference there…
For profit medicine and for profit health insurance is just riddled with moral hazard.
There is legal precedent establishing healthcare providers' obligations in life-threatening situations. The same moral responsibility should exist when insurers deny lifesaving care, it's just hidden behind bureaucracy.
Depends on your philosophy I suppose. For example, Christianity teaches that failing to do good is itself a sin. So that suggests that an omission could be considered to make someone guilty.
I suspect that all modern legal systems have the concept of negligence which could result in someone being considered guilty for someone's death. I imagine in that case whether that's "murder" would come down to whether you mean a legal definition (which might call it something else like "manslaughter") or the colloquial definition.
And guilt isn't a single bucket or item to be handed out to one person. Most if not all moral systems and laws admit of varying degrees of responsibility and culpability and work within that framework (see situations where a bank robbery goes wrong and one robber kills someone and the getaway driver is also charged as an accessory to the killing).
The doctor / hospital that refuses to treat when insurance declines is also involved in the “omission of expected care”. Would they also be guilty of premeditated murder?
Also without this murder, we could imagine that the NYPost would have never written this article to alert on the malfeasance of healthcare providers...
Why wouldn't they do their part as a news org, and why did they wait for the murder to publish such an article, if that murder was not "needed" for things to change, then?
One issue is that if denying medical care is murder then every healthcare system is guilty.
In the US it’s insurance companies (or the government through Medicare or Medicaid) but in the UK it’s NICE, in Canada it’s CADTH and the provincial health authorities.
Since there are finite resources spent on healthcare, trade offs are made all the time. If spending $10M on treatment A saved 10,000 lives and $10M on treatment B saves 1,000 lives, then treatment A gets funded and treatment B doesn’t.
The difference is that patients in the US have an up close and personal experience with denial.
In Canada and the UK they don’t because doctors knows what is covered and what isn’t so never bring up life saving options if they aren’t paid for.
In rare circumstances like cystic fibrosis in the UK, patients become aware that they are being denied a life saving drug and protest, but generally it’s pretty rare because patients just don’t know the option exists.
The difference is that patients in the US are being denied by people lining their own pockets with the savings. In sane countries, there’s at least some basis of trying to do the most good with the resources at hand, which sometimes means denying care for person A because those resources would be better spent on person B. With private insurers in the US, it means denying care for person A because they think they can get away with it and it will increase their profits.
If you actually trace the cashflows, the "people lining their own pockets with the savings" are mainly not the insurers but rather the executives and shareholders for other large companies with self-funded employee health plans. Most insurance companies no longer provide much real insurance but rather primarily administer health plans on behalf of self-funded employers. Due to the minimum medical loss ratio rule, insurers actually make more profit the more claims they approve.
If employers wanted it, insurers would be happy to offer health plans that fully paid every claim with zero denials. This would be enormously profitable for the insurers because they could run those health plans with minimal work. But instead, most employers are constantly looking for ways to cut employee health benefit costs. This means incentives aren't aligned.
> With private insurers in the US, it means denying care for person A because they think they can get away with it and it will increase their profits.
The person at the insurer who denies a claim is not making more money because they denied it. The company as a whole might, but not the person denying it.
The US spends the most budget per patient for the least amount of care, the rest goes into inefficiency and profit (a second kind of inefficiency).
Medicare per-capita spending is more than NHS per capita spending, but the NHS covers everyone.
Of course healthcare is denied in any system (in other systems this is triage), but nowhere to the level United Health does it: over 30%, it's on a completely different scale.
Your argument is completely bogus for multiple reasons. Firstly, people are paying here for insurance, a lot. Secondly, it's the FDA's job to approve treatments which it does. Thirdly, we do not have a uniform privatized determination across the country of what is approvable or not by insurance companies. They deny numerous legitimate treatments and procedures at their whim.
Plenty of treatments are denied in other countries. Not to mention most other countries have private insurance layered on top of public and it’s the same issue - private insurers denying a treatment through their own process.
If US insurers are guilty of murder than most of the worlds insurers are too.
>Well, if a killing is ethically justified, it isn't murder.
Are you saying this as an opinion, or is this an established thing? I thought murder was an "unlawful killing without justification or valid excuse" (paraphrased from Wikipedia), whether one finds it ethical or not is sort of beside the point. Especially because there is no objectively correct ethics.
But, I'm not a lawyer, this is just my understanding.
I would say you have to be careful and specific - as "murder" is usually the domain of the law and "ethically justified* is the domain of ethics.
It's quite easy to come up with situations where the law declares a killing as unequivocally murder yet everyone agrees it was ethically justified. The opposite can happen too.
"Murdering a murderer to save many innocents could be considered ethical by some?"
This is a heavy statement.
More I read, heavy it gets.
Kill people it never the answer. The ideia that "I" have the power is weak. People, together, have power, however they don't know what to do. In his case the easiest way to win is pressuring the government, with the people, for clear changes.
the article cites a study that says: "5% of practitioners reported anesthesia times greater in total than what would be expected across university, community, and specialty hospitals. Furthermore, it was found that the greatest differences in expected anesthesia times were in specialty hospitals compared with university hospitals.8 However, the authors have stressed that their findings should not be interpreted to indicate fraud because fraud involves intent, which could not be determined. Because this study was a retrospective study, the authors could not rule out the alternative but unlikely explanation that the practitioners could be rounding down. The reason for caution by the authors is that the CMS has differentiated fraud from abuse by emphasizing that fraud is intentional, whereas abuse is the result of poor medical practices.2 This differentiation is important because sometimes the rounding in digits ending in 0 or 5 minutes in anesthesia time is part of the organization culture of operating rooms in which rounding is performed systematically by the operation room circulating nurse along with the anesthesia practitioner. Sun et al8 recognized this issue as being related to institutional factors, which was one of the reasons they performed a 2-step regression analysis; long anomalous times were not sufficient to establish inappropriate discretion.8"
So Anthem based on the article it might be overpaying for at worst 5% of the operations BUT the big but is that in some hospitals it is routine to round digits. So paying less workers for some rounding operations? It doesn't look as bad to me. It might be because of reasons, or might be due to media backslash.
I think it's safe to assume we definitely need more research into healthcare companies rules after healthcare companies ceo related killing
I find absolutist stances based on ideology distasteful. History has pretty vividly shown that sometimes killing people is in fact the answer. Something something Nuremburg trials.
I hate the way the press and seemingly most people are approaching this but am completely unsurprised: "You are either a heathen who supports murder or you are a virtuous supporter of the people and this man deserved to die." Two things can be correct at the same time. 1) Murder is not OK. 2) The insurance industry is completely broken as it incentivizes terrible behavior and this CEO was a scumbag who perpetuated this behavior while possibly insider trading.
You can't just shoot people and kill them in the street! That's barbaric! You need to do it from behind a desk through a corporate bureaucracy like a civilized person.
I guess we aren't going back in time to kill Hitler any more then?
The media pearl-clutching is extremely heavy this time around, painting Luigi as an unhinged lunatic and all the rest. It feels incongruent and purposefully dismissive to equate this to something like the Oklahoma City Bombing.
Given the NY Posts leanings I’m not surprised they walked that line by putting it in there.
Media seems to be on an agenda setting tear to disavow the murder, but I think it’s a frankly boot licking response to what is going on here.
I think this spooked a lot of executives (re: “elites” if you will) and there is pressure to ignore the nuance of what the murder means to people and why it isn’t the same as say, stabbing a tech CEO in SF like what happened last year
The American people need to stop seeing the other party as the enemy. As long as that’s in place, the parasites at the top will remain in power.
Unfortunately, it’s easy for them to create conditions to perpetuate and widen the American political schisms. And they’ve convinced both sides the common historical solutions (nationalism, limited democracy, religion) are for low IQ bigots. Things are likely too far gone.
Consider what happened with the public option in Obamacare. Both parties played a part in defeating it. The Democrats’ part was that they had 59 Senators in support, and one single dude opposed. The Republicans’ part was that they had 40 opposed and none in favor. Because a 60% majority was required, it failed.
That does not look to me like both sides are at fault and we need to think of it differently. That looks to me like Democrats are imperfect but largely aligned with what I want, whereas Republicans are resolutely in opposition.
The slain CEO was a Democrat, like many of his peers. Again, it's not about political party. Red vs Blue partisan theatre is a tool used by the united ruling class to divide the exploited classes.
Here's my semi-cooncrete mechanism. Seniors seem to love Medicare...
Every year for 10 years, reduce the age of eligibility by 1 year. At N+10, it will cover 55+.
For the next 10 years, reduce the age of eligibility by 2 years per year. At N+20, it will cover 35+.
You can also set up Medicaid to cover all children in a similar way (after all, most children have no income, so should qualify if judged on personal income rather than family income). Set a date and if you're born after that date, you get medicaid until you're 20.
At year N+20, there will be a 15 year gap for young people. Which is hopefully time enough for them to earn enough social security credits to qualify for Medicare.
And yes, medicare and medicaid taxes would have to go up. But private healthcare premiums should go down.
Rolling it out over 20 years allows for adjustments to be made as things go along. Criteria based on years is for simplicity... A better method would be increasing eligible population by 1% the first year, 1.1% the second, and so on until you're done.
If people really don't want to just pay for it socialized. Just make it possible to self pay for medicare at more ages; this is something that seniors without enough social security credits can already do. Again modulating the eligible age over time to allow for a transition without overwelming the system.
>Give me universal health care...but don't increase my taxes!
Yeah, why not? The US already spends more tax dollars per person in healthcare. The excess gets funneled to the insurance companies. There's no reason why we can't implement universal healthcare without increasing taxes.
Well, the events you are seeing unfolding is change around the established systems.
Civil disobeyance is nothing new. The fact that is is so little pronounced currently is probably a signal that there has been alignment for quite a while.
Bit when politicians do not take their jobs seriously, change finds other ways.
I thought it was because of Joe Lieberman, a Democrat turned independent, from a state that tries to bill itself as the "Insurance Capital of the World" [2]
If it had been 39 Republicans, it would have been 2 Democrats.
Obama campaigned for Joe Lieberman afterwards as an independent against Ned Lamont, who had won the Democratic primary. Lieberman tanked the public option for the Democrats, and Obama was paying his debt.
Democrats would have paid the price at the polls for getting rid of the public option. Lieberman took the hit for the rest of them; he was the cheapest, because he already publicly held right-wing positions. If they had needed another vote, they would have had to find another Democrat to risk their political career to do it. Probably with a cushy lobbyist job at a health insurer after getting voted out.
There are lots of people who get freaked out and go to the hospital for every little thing. We used to have a term for that: "hypochondriac." Now it's become socially acceptable, so you don't hear the term as much.
Everyone knows Americans pay the most for medical treatment, but the life expectancy is not that high. If you know your behavior isn't good for you, but you can't stop yourself, well, that's an addiction.
On the contrary, if the healthcare system in the US weren't such shit, more people would probably be going to primary care doctors and getting Preventative Care before it becomes an emergency, and requires a trip to the hospital.
But many people don't, because visiting a primary care / walk-in clinic / urgent care is expensive, so they ignore it, until it becomes un-ignorable. Now it's an ER visit.
> Everyone knows Americans pay the most for medical treatment, but the life expectancy is not that high.
Sure.
> If you know your behavior isn't good for you
This doesn't follow. Our healthcare system might be worse than some but that does not imply it's bad for you. That same logic would imply getting punched in the face is good for you because it's better than getting shot.
I was thinking about condensing my thoughts into a post, but I'll make one point on the issue of premiums. In the article, it says the cost of insuring a family of four is $25,000 a year. That sounds accurate to me.
I know from experience (being self-employed for a period of time and having to figure this all out myself) that if your family is healthy, you can replace all 4 full-term plans with 4 short-term plans and pay about $4,000 a year for the same coverage. The only difference, really, is that your insurance coverage ends after one year and you have to apply for it again. This used to be seen as risky, but with the ACA, someone will always be forced to insure you. So, it's not the same anymore.
That's not even all we could collectively do to solve this problem. Just imagine if all the healthy people in America just did that. I know, there aren't many healthy Americans left. And a lot of people have health insurance as part of their benefits package.
But many of those people are paying their dependents' insurance out of pocket. So, someone on a full-term plan could switch all his dependents to short-term and save about $5k per year per person. And it doesn't cause any noticeable difference to someone's coverage.
Imagine if only 1 million healthy Americans went from full-term to short-term. The health insurance industry would lose 5 billion dollars of income a year. That's not huge for a $500B industry, but it's not nothing. Corporate America sits up and starts paying attention to what's going on at ANY loss of revenue.
This is not insurance advice, but just thinking out loud. Verify everything yourself, but my point is that there's a lot everyday Americans could do to hurt these companies in their wallets. We just need to come together, share ideas, and trust ourselves and each other more than nameless, faceless companies.
Here's a goalpost for you: a healthy person should not spend more than $2,000 a year, total, on any health care related expenses. Even that number is ridiculous. But it's probably about half of what people are paying. If we all focused on that, and helped each other achieve that totally achievable goal, we'd change a lot about this rotten system.
I’m against vigilante killings because I don’t want to live in that kind of a society. But a couple days later, Anthem decided to end their insane time limits on anesthesia. I’m hoping the public’s reaction to all these events has put a bug in the ear of politicians who ran partly on the idea of “repeal the ACA”: maybe this isn’t a great time to start slashing coverage. People seem pretty upset about it right now.
I agree with your general points, but if we can trust Vox, the Anthem situation wasn't quite what people thought. The policy was to prevent overpayment to anesthesiologists, because they get paid partly by the hour and there's evidence that they tend to inflate their times. The policy would not have increased costs to patients, because of this:
> “Say there is a contract between an insurance company like Anthem and an anesthesiologist,” Garmon told Vox. “What is always in that contract is a clause that says, ‘You, the provider, agree to accept the reimbursement rules in this contract as payment in full.’ That means the provider cannot then turn around and ask [the patient] for money.”
There was also a process for anesthesiologists to apply for extra payment if surgery went extra long.
They make a larger point that the main reason Americans pay so much more for healthcare is that we pay our providers a lot more. Nations with more reasonable costs and high-quality results have controls in place to keep costs down at the provider level.
Vox might be right but under no circumstances would a company admit "hey we're changing this unpopular decision because we're personally afraid of being killed". Tying good patient outcomes to dead CEOs would be literally suicidal for Anthem execs.
They know. They don’t care because they think it doesn’t affect them. They’ve largely been right so far. But this should be their sign to fix it before discontent boils over.
Most people in positions of power realize that it's bad in some ways and good in others. It's bad in cost effectiveness and universal access to affordable primary care. It's (relatively) good at other things like 5-year cancer survival rates, waiting times for elective treatments, trauma care, and drug development. There is little agreement on how to fix the bad while preserving the good.
I don't know what happened but this super duper upvoted post disappeared from the home of hn. perhaps moderators temporarily shadow content that is upvoted too much? Or else?
Also curious about this. Several other posts of similar age and with fewer points are in top spots on the front page. This post is still gathering comments, but seems to be hidden.
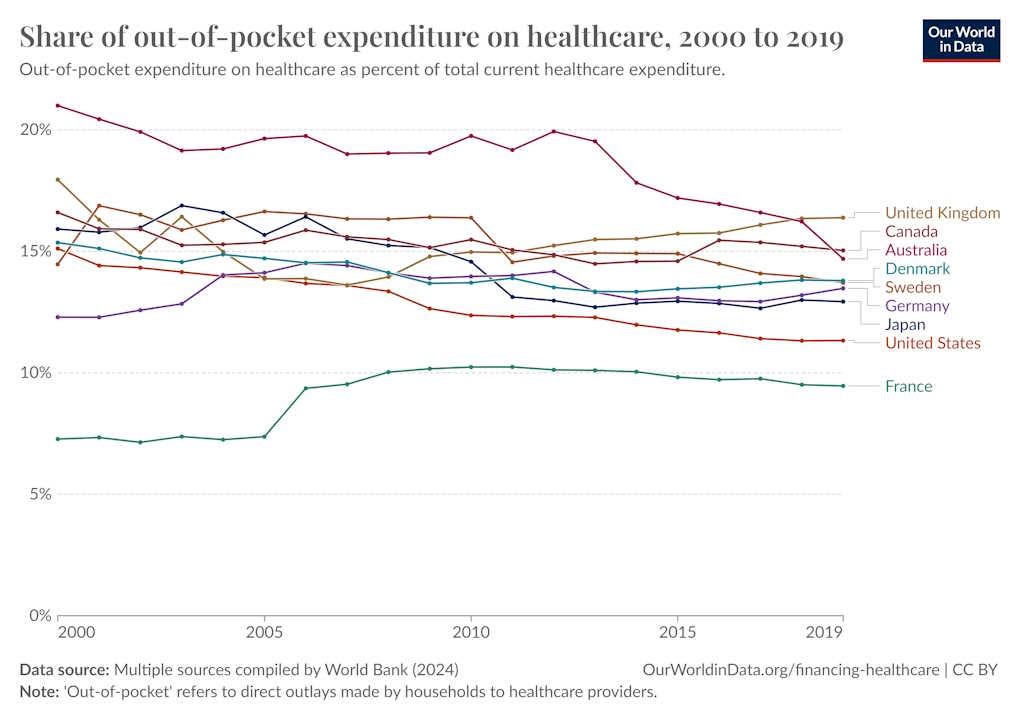{kind=link}
Additionally, it reports that denial rates have increased 10x in 10 years, based on the following chain:
- "UnitedHealthcare nixed 1.1%, Humana 1.9%, Aetna 1.5% in 2013, per the American Medical Association."
- "By 2022, major insurers were refusing to pay, on average, 15% of claims, according to a national survey of hospitals and health-care providers by Premier, an insurance consultant."
- "The figure continues to shoot upward, with some companies today denying almost _half_ of all claims, according to researchers at the Kaiser Family Foundation."
Furthermore, "few people appeal, but of those that do 41% obtain a reversal", which suggests the denials may be unfair.
I certainly would like to know the denial rates when selecting an insurance provider. As the article says, "You aren't really insured if your insurer can deny valid claims with impunity."
Given that the ACA requires this information be provided, it certainly ought to be provided. Then we'd have a much clearer picture.
It's an opinion piece on a news site known for inflammatory articles but it reports some interesting information. It would be much nicer if it included references to the research it's based on, but it seems pretty reasonable to me.